
What's on this Page
Is Colon Cancer Curable? New Research Shows 90% Survival Rate in Early Detection

Is colon cancer curable? The answer is encouraging when detected early, with localized colon cancer showing a remarkable 90% five-year survival rate. This stands in stark contrast to advanced stages of the disease, where survival rates drop significantly.
Colorectal cancer ranks as the third most common cancer diagnosis in both men and women in the United States. While this statistic might sound alarming, there’s good news. The incidence and mortality rates from colon cancer have been steadily declining over the past several decades, falling on average 2.4% each year. This decline is largely due to improved screening methods and earlier detection.
When we look at survival rates by stage, the differences are striking. The overall five-year survival rate for colorectal cancer patients (all stages included) is 65%. However, this rate varies dramatically based on how early the cancer is detected. Localized disease has a 91% survival rate, compared to just 13% for distant cancer that has already spread.
In this article, we’ll explore what colon cancer is, its symptoms, causes, and treatment options. Most importantly, we’ll discuss the critical role of early detection in improving curability and how recent research supports the 90% survival rate in early-stage diagnosis.
Understanding Colon Cancer and Its Curability
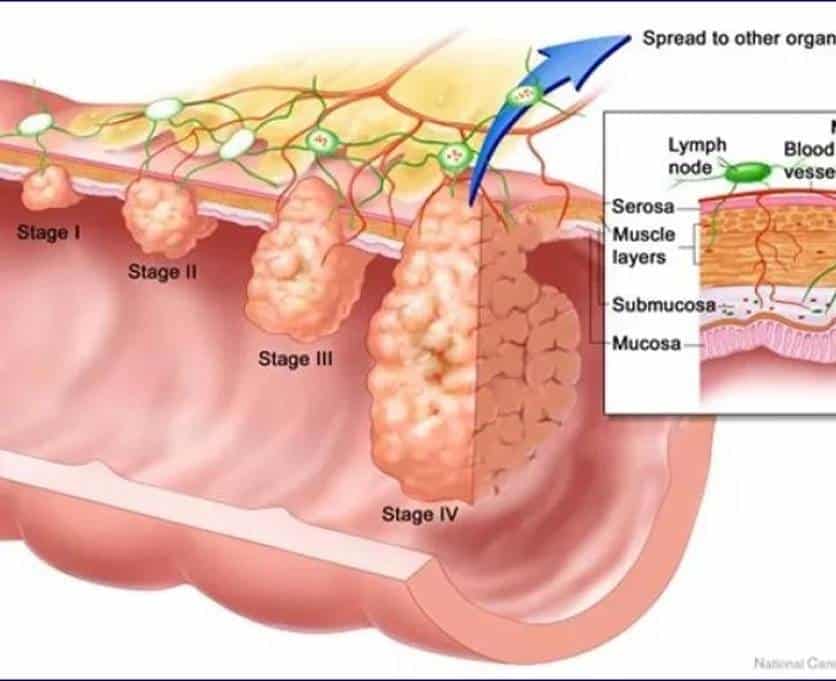
Image Source: Colon Cancer Alliance
Understanding the difference between types of intestinal cancers is crucial for patients and their families. Colorectal cancer encompasses a broader category that includes both colon and rectal cancers, although these terms are sometimes used interchangeably [1].
What is colorectal cancer vs colon cancer?
The colon and rectum make up the large intestine, forming distinct but connected parts of our digestive system [2]. Specifically, the colon constitutes the first five feet of the large intestine, primarily absorbing water from stool [2]. In contrast, the rectum makes up the final six inches, storing stool until elimination [2].
Despite their anatomical proximity, these cancers differ in important ways. Notably, rectal cancer has approximately a 20% risk of local recurrence, whereas colon cancer has only about a 2% risk [3]. This difference exists primarily because the rectum lacks the protective outer layer (serosa) that surrounds the colon, making it easier for tumors to break through and spread locally [3].
Treatment approaches also differ between these cancers. For colon cancer, surgery typically comes first, potentially followed by chemotherapy [3]. Alternatively, rectal cancer treatment often begins with chemotherapy or radiation to shrink the tumor before surgical removal [3].
Adenocarcinoma of colon: the most common type
Among colon cancer types, adenocarcinoma predominates, accounting for approximately 95% of all cases [4]. This cancer originates in the gland cells that produce mucus to lubricate and protect the inner lining of the colon and rectum [5].
Adenocarcinomas typically develop from polyps – abnormal growths within the inner lining of the colon [1]. Most colorectal cancers evolve through a protracted multistage process spanning several decades [6]. Furthermore, this progression from polyps to malignancy typically takes 5-15 years, creating an opportunity for early detection and prevention [6].
Pathologists classify colon adenocarcinomas into three grades:
- Well-differentiated (low grade)
- Moderately differentiated (intermediate grade)
- Poorly differentiated (high grade) [5]
The grade matters because poorly differentiated cancers tend to grow and spread more quickly than well or moderately differentiated ones [5]. Additionally, other factors like genetic mutations and the extent of spread also impact prognosis and treatment decisions.
Is colon cancer curable in early stages?
The encouraging news is that colon cancer detected early is highly treatable and often curable [4]. Surgery serves as the primary treatment for colon cancer and results in cure for approximately 50% of patients [4].
Curability correlates strongly with the cancer’s stage at diagnosis. For stage I colon cancer, surgery alone achieves an impressive 95% five-year disease-free survival rate [6]. Similarly, stage II colon cancer treated with surgery alone shows 82-88% five-year disease-free survival rates [6].
Even for stage III patients, surgery alone can achieve 45-50% five-year disease-free survival rates, which improves to 67-70% with the addition of oxaliplatin-based adjuvant chemotherapy [6]. Essentially, this means about 17-20% of stage III patients survive long-term specifically because of chemotherapy [6].
At specialized centers like MD Anderson, local recurrence rates for colon cancer are remarkably low – less than 1% – primarily because surgeons achieve clear surgical margins and complete resection of all tumor-associated lymph nodes during initial surgery [1].
Most patients successfully treated for colon cancer can expect to resume normal lives. In fact, some patients with stage I colon cancer have demonstrated longer lifespans than the general population [1]. Moreover, for patients with more advanced disease who achieve cure without recurrence, life expectancy typically approaches normal [1].
Regular screening remains vital since approximately 75% of newly diagnosed colorectal cancer patients present with non-metastatic early-stage disease, creating opportunities for curative-intent treatment [6]. When found in early stages, the five-year survival rate reaches about 90% [1].
How Colon Cancer Develops Over Time
Image Source: ResearchGate
“Fortunately, colon cancer is relatively slow-growing, with benign (noncancerous) polyps typically taking approximately 10 to 15 years to develop into cancer.” — Moffitt Cancer Center, National Cancer Institute-designated comprehensive cancer center
Colon cancer typically develops through a gradual progression that spans many years. The transformation from healthy colon tissue to invasive cancer follows distinct pathways with specific genetic changes at each step. Understanding this progression helps explain why early detection dramatically improves survival rates. From polyps to malignancy: the adenoma-carcinoma sequence
The journey from normal colon tissue to cancer typically follows what scientists call the adenoma-carcinoma sequence. This process begins with the formation of benign polyps that, if left untreated, may eventually transform into invasive cancer. The progression typically unfolds over 5-15 years, creating an opportunity window for early detection [3].
The sequence generally progresses as follows:
- Initial genetic alteration – Often occurring in the APC gene on chromosome 5, giving affected cells a growth advantage
- Polyp formation – Abnormal cell growth creates small, benign growths
- Adenoma development – Polyps grow larger with increasing risk of malignancy
- Accumulation of additional mutations – Particularly in genes like KRAS, TP53, and DCC
- Transformation to carcinoma – Invasion beyond the colon’s inner lining
Not all polyps carry the same risk. Adenomatous polyps can be classified into three histological types with increasing malignant potential: tubular, tubulovillous, and villous [7]. Among these, villous adenomas pose the highest risk for malignant transformation. Furthermore, larger polyps (especially those over 1 cm), polyps with villous components, and those showing high-grade dysplasia carry greater malignancy potential [7].
Genetic mutations and mismatch repair pathways
Presently, colorectal cancer development follows three primary molecular pathways, each characterized by distinct genetic alterations:
Chromosomal Instability (CIN) – This pathway accounts for approximately 65-70% of sporadic colorectal tumors [5]. CIN tumors show widespread chromosome number alterations (aneuploidy) and frequently lose portions of chromosomes 5q, 18q, and 17p, which contain important tumor suppressor genes [7]. About 60% of CIN tumors contain inactivating mutations in TP53 [5].
Microsatellite Instability (MSI) – Found in roughly 15% of colorectal cancers [5]. MSI occurs when the DNA mismatch repair (MMR) system—responsible for correcting errors during DNA replication—malfunctions [8]. This leads to accumulation of mutations, particularly in repetitive DNA sequences called microsatellites. MSI tumors have 10 to 100 times more somatic mutations than MSI-stable tumors [9].
CpG Island Methylator Phenotype (CIMP) – This pathway involves abnormal DNA methylation, which can silence important tumor suppressor genes [7].
An early and critical event in most colorectal cancers is the loss or inactivation of the APC gene [7]. Other key mutations include KRAS (found in nearly 40% of colorectal tumors [5]), PIK3CA (18%), FBXW7 (14%), SMAD4 (14%), and BRAF (10%) [5].
What causes colon cancer in females and males?
Consequently, the development of colon cancer in both sexes primarily results from a combination of genetic and environmental factors. Generally, only about 5% of colorectal cancers stem directly from inherited genetic syndromes [6], with most cases classified as “sporadic.”
Risk factors common to both sexes include:
- Age – Most people diagnosed are over 50, though cases in younger individuals are increasing [10]
- Family history – Having first-degree relatives with colorectal cancer increases risk [1]
- Inflammatory bowel disease – Conditions like ulcerative colitis and Crohn’s disease increase risk [1]
- Lifestyle factors – Obesity, smoking, and regular alcohol consumption contribute to risk [10]
Particularly noteworthy, research shows that men face approximately 50% higher risk of developing colorectal cancer than women [6]. Young women (18-44 years) with colorectal cancer generally have better survival chances than men of the same age [6].
Inherited syndromes like Lynch syndrome (hereditary non-polyposis colorectal cancer) account for 2-4% of all colorectal cancers [1]. People with Lynch syndrome have up to 50% lifetime risk of developing colorectal cancer [11]. Women with Lynch syndrome face additional risks, including high rates of endometrial cancer [1].
Recognizing Early Symptoms and Warning Signs
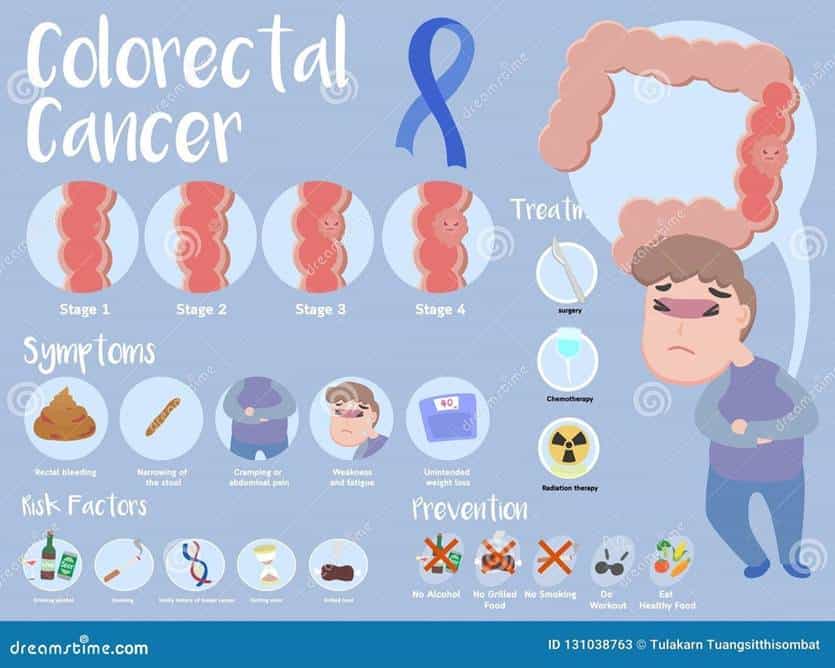
Image Source: Dreamstime.com
Recognizing symptoms early remains crucial for improved colon cancer outcomes. Yet many patients face significant delays between initial warning signs and final diagnosis. According to recent research, recognizing certain key symptoms could potentially help catch the disease at an earlier, more treatable stage.
Stage 1 colon cancer symptoms
Stage 1 colon cancer typically produces minimal or no noticeable symptoms, making it challenging to detect without screening. Indeed, this represents one of the greatest challenges in early diagnosis. “Early-stage colon cancers are generally small cancers that are only in the colon. Many people with these cancers have no symptoms,” experts emphasize [12].
As a result, routine screening tests become vitally important. These tests often detect disease before symptoms develop, highlighting their significance in early diagnosis and effective treatment. For patients who do experience symptoms, they often include:
- Blood in the stool (either bright red or making stools appear darker)
- Changes in bowel habits lasting more than a few days
- Abdominal pain or discomfort
- Unexplained fatigue or weakness
First thing to remember: these symptoms frequently overlap with common conditions like hemorrhoids, irritable bowel syndrome, or digestive infections. Accordingly, many people initially dismiss them, contributing to diagnostic delays.
Symptoms of colon cancer in women vs men
Contrary to what some might assume, colon cancer symptoms do not differ significantly between men and women. “What are the symptoms of colorectal cancer in women? They’re actually the same for everyone, regardless of gender,” note cancer specialists [13].
The most common symptoms across both sexes include:
- Blood in the stool
- Unintentional weight loss
- Persistent constipation or diarrhea
- Excessive fatigue
- Abdominal pain or cramping [13]
Nevertheless, symptom presentation can vary based on tumor location rather than gender. Left-sided cancers (in the descending colon, sigmoid colon, and about one-third of the transverse colon) typically cause bowel habit changes and visible blood in stool. Conversely, right-sided cancers often lead to iron deficiency anemia, fatigue, and weight loss [12].
For women, it can occasionally be challenging to differentiate between certain symptoms. Cramping, bloating, or bleeding might initially be attributed to menstrual issues rather than potential colon cancer [13]. Therefore, women should pay close attention when abdominal pain differs from typical menstrual discomfort or persists longer than a normal period.
Mass in colon: when to investigate
A mass in the colon represents a significant finding that warrants prompt medical evaluation. Patients may occasionally feel a lump in the abdomen or rectum [2], though this typically occurs in more advanced stages. More commonly, a mass is detected during medical examinations or diagnostic imaging.
Healthcare providers might feel your abdomen for masses or organs larger than normal or perform a digital rectal exam [14]. Should they detect an abnormality, further investigation becomes necessary.
Several warning signs suggest the need for immediate investigation:
- Rectal bleeding or blood in stool
- Persistent abdominal pain
- Unexplained weight loss
- Significant changes in bowel habits
Research indicates that having just one of these warning signs during the period of 3 months to 2 years before diagnosis was associated with nearly twice the likelihood of being diagnosed with early-onset colorectal cancer. Furthermore, having three or more signs was associated with six times the likelihood of diagnosis [4].
Undoubtedly, early recognition and prompt investigation of these symptoms significantly improve outcomes. For colorectal cancer caught at a localized stage, 5-year survival reaches an impressive 90%, compared to only 14% for cancer that has spread to distant organs [4].
Staging and Its Role in Curability
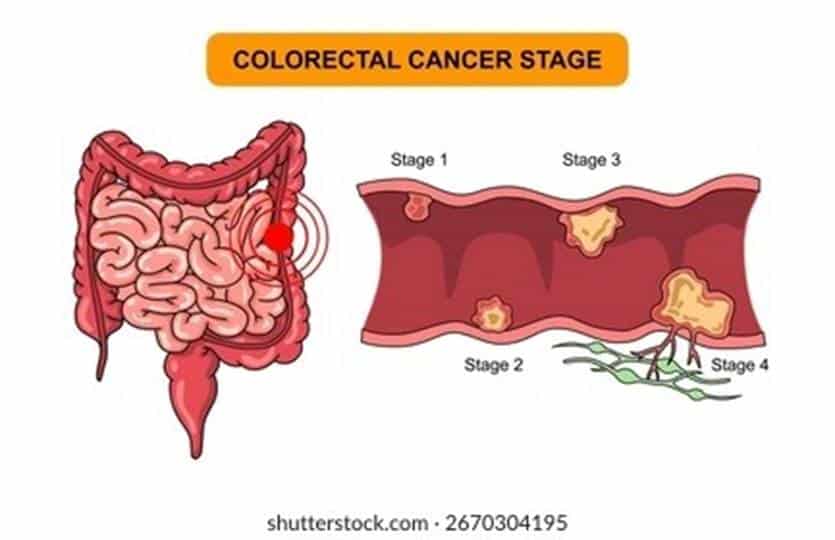
Image Source: Shutterstock
“The five-year survival rate for CRC is approximately 91% for stages I and II but declines to 13% for stage IV.” — Colon Cancer Coalition, National nonprofit organization dedicated to colon cancer awareness and prevention
Cancer staging profoundly influences treatment decisions and predicts potential curability for colon cancer patients. Staging tells doctors exactly where the cancer is located, whether it has spread, and how far it has advanced—serving as the roadmap for treatment planning. At what stage is colon cancer curable?
Colon cancer curability varies dramatically based on the stage at diagnosis. The staging system ranges from 0 to IV, with lower numbers indicating less advanced disease that hasn’t spread far from its origin.
Stage 0: Cancer remains confined to the innermost lining of the colon (mucosa). At this stage, surgical removal of the cancerous tissue—often accomplished during colonoscopy if the polyp is completely removed with clear margins—typically results in cure with no additional treatment needed [5].
Stage I: Cancer has grown deeper into the colon wall but hasn’t spread beyond it or reached lymph nodes. For patients with stage I, surgery alone provides excellent outcomes, with approximately 95% five-year disease-free survival rates. Most stage I patients require only surgical removal of the affected section of colon (partial colectomy) [5].
Stage II: Cancer has penetrated through the colon wall and possibly into nearby tissue, yet lymph nodes remain cancer-free. Surgery remains the cornerstone of treatment, alongside nearby lymph node removal [5]. Stage II has three substages (IIA, IIB, IIC) depending on how far the cancer has grown through the colon wall [15].
Importantly, the five-year survival rate for localized colon cancer (stages I-II) reaches an impressive 91% [16], highlighting the critical importance of early detection.
Is colon cancer curable at stage 3?
Stage III colon cancer occurs when cancer cells reach the lymph nodes near the tumor but haven’t spread to distant body parts [17]. Although this represents more advanced disease, stage III colon cancer is still potentially curable for many patients.
Standard treatment involves:
- Surgical removal of the affected colon section (partial colectomy)
- Removal of nearby lymph nodes
- Adjuvant chemotherapy (typically FOLFOX or CAPEOX regimens) [5]
The outlook for stage III patients continues to improve with medical advancements. Surgical resection alone may cure approximately 50% of people with stage III colon cancer, while adjuvant chemotherapy benefits an additional 30% of patients [17]. Subsequently, about 72-73% of patients with regional colon cancer survive at least five years after diagnosis [16].
Recent research indicates that some stage III patients may need only 3 months of adjuvant chemotherapy rather than the traditional 6 months, depending on specific cancer characteristics [5].
Is stage 4 colon cancer curable?
Stage IV (metastatic) colon cancer has spread beyond the colon to distant organs—primarily the liver, lungs, or abdominal cavity lining [18]. Henceforth, the five-year survival rate drops to approximately 13-15% [16].
Nevertheless, stage IV colon cancer may be curable in select situations:
- When there are only a few small metastases in the liver or lungs that can be surgically removed alongside the primary tumor [5]
- Following successful treatment with chemotherapy to shrink initially inoperable metastases [5]
- In certain cases where liver transplantation is an option [7]
“An estimated 20% of patients with metastatic colorectal cancer are alive 5 years after receiving a diagnosis,” notes recent research [7]. This represents significant progress, as previously only about 1% of stage IV patients lived that long.
Newer treatments offering hope for stage IV patients include:
- Targeted hepatic artery infusion (HAI) therapy delivering concentrated chemotherapy directly to liver metastases
- Immunotherapy for tumors with specific genetic characteristics
- Liver transplantation for carefully selected patients [7]
Throughout all stages, specialized cancer centers achieve superior results. At MD Anderson, for instance, local colon cancer recurrence rates remain below 1%, primarily due to achieving clear surgical margins and complete lymph node removal during initial surgery [11].
Treatment Options Based on Stage
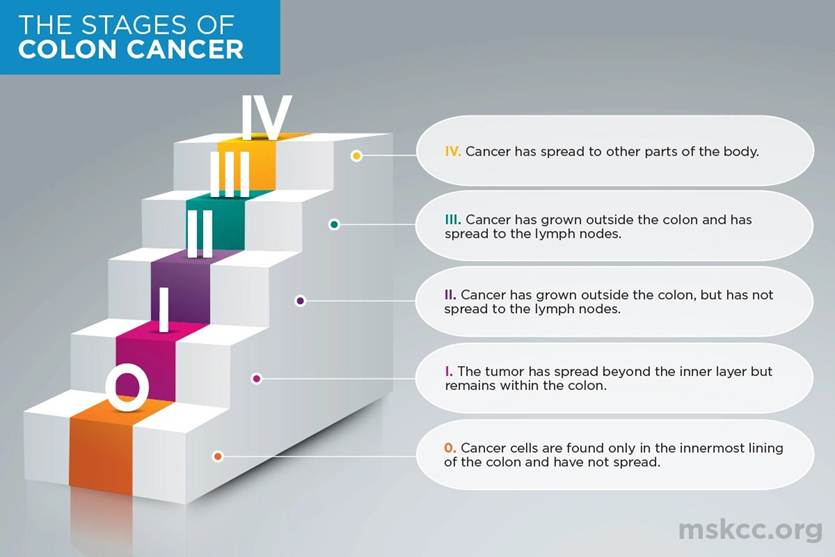
Image Source: Memorial Sloan Kettering Cancer Center
Treatment approaches for colon cancer vary significantly depending on disease stage, tumor characteristics, and patient health. The treatment landscape continues to evolve, offering increasingly effective options even for more advanced disease.
Is colon cancer curable after surgery?
Surgery serves as the cornerstone of treatment for most colon cancer patients, especially those with localized disease. For many, it offers the possibility of complete cure. Surgical removal of the affected colon section (partial colectomy) alongside nearby lymph nodes remains the primary intervention for stages 0-III [5].
Studies define “cure” as 5-year survival without recurrence, with an overall cure rate of 65% among colon cancer patients [19]. The cure probability varies markedly by stage—patients with stage I disease have a 91% cure rate, versus 64% for stage III [19]. At specialized centers like MD Anderson, the local recurrence risk after surgery is remarkably low at less than 1%, primarily due to achieving clear surgical margins and complete lymph node removal [11].
Notwithstanding these promising statistics, recurrence risk persists. Most recurrences (60-80%) emerge within 2 years after surgery, with 95% appearing within 4 years [19].
Chemotherapy and targeted therapy for stage 3 and 4
Stage III patients typically receive adjuvant chemotherapy following surgery. Common regimens include FOLFOX (5-FU, leucovorin, and oxaliplatin) or CAPEOX (capecitabine and oxaliplatin) [5]. Recent research indicates that 3 months of chemotherapy might be sufficient for some stage III patients rather than the traditional 6 months [5][9].
For stage IV (metastatic) disease, treatment options expand beyond surgery to include:
- Combination chemotherapy regimens: FOLFOX, FOLFIRI, CAPEOX, or FOLFOXIRI [5]
- Targeted therapies directed at specific genetic features
- Liver-directed treatments for hepatic metastases [8]
Targeted therapy has become increasingly important in metastatic disease. Options include anti-VEGF drugs like bevacizumab that block blood vessel formation, and anti-EGFR agents such as cetuximab and panitumumab for patients with RAS wild-type tumors [18].
Role of immunotherapy in MSI-high tumors
Perhaps the most exciting advancement involves immunotherapy for microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) tumors. These genetic features appear in approximately 5% of metastatic cases and 15% of early-stage colorectal cancers [20].
Immune checkpoint inhibitors like pembrolizumab (Keytruda) and nivolumab (Opdivo) have shown remarkable efficacy in these patients. In the KEYNOTE-177 trial, pembrolizumab as first-line treatment for MSI-H/dMMR metastatic colorectal cancer achieved a 40% response rate with improved progression-free survival compared to chemotherapy [21]. After 24 months, 48.3% of patients receiving pembrolizumab remained progression-free, versus just 18.6% with standard chemotherapy [21].
Similarly impressive, the combination of nivolumab plus ipilimumab demonstrated a 69% objective response rate with 13% complete responses in the CheckMate 142 study [21].
Most strikingly, a clinical trial at Memorial Sloan Kettering Cancer Center reported that 100% of participants with MMRd rectal cancer who received immunotherapy saw their tumors disappear—without requiring surgery, chemotherapy, or radiation [8].
Through these advances, colon cancer treatment continues to improve, offering hope even for patients with advanced disease.
New Research on Early Detection and 90% Survival Rate
Recent advances in screening technology have fundamentally altered the outlook for colon cancer patients. Early detection stands at the center of these improvements, offering not just treatment but often complete prevention of the disease.
How early detection improves outcomes
The evidence supporting early detection is compelling—colorectal cancer caught in early stages (1 & 2) has a survival rate of approximately 90% [1]. This stark contrast becomes evident when compared to advanced stages, where the five-year survival rate for distant colorectal cancer drops to just 13-14% [6][22].
Throughout the disease progression, a critical window of opportunity exists. Colorectal polyps typically take 10-15 years to develop into cancer [10], creating an extended timeframe for intervention. Effectively, screening not only detects existing cancers but often prevents them by identifying and removing precancerous growths before they become malignant.
Alongside improved survival outcomes, early detection offers additional benefits: less invasive treatment options, fewer complications, and reduced healthcare expenses [23]. Many early-stage cancers require only surgical removal without the need for additional treatments like chemotherapy or radiation.
Recent studies on survival rates by stage
Current research confirms striking differences in survival rates based on stage at diagnosis:
- Localized disease (Stages 0-II): 91% five-year relative survival rate [6]
- Regional spread (Stage III): 73-74% five-year relative survival rate [6][22]
- Distant metastases (Stage IV): 13-18% five-year relative survival rate [6][22]
The United States has seen both decreased incidence and mortality from colorectal cancer, primarily attributed to improved screening methods [22]. Ultimately, these statistics underscore a critical point: almost 60% of colorectal cancer deaths could be prevented with appropriate screening [3].
Screening methods: colonoscopy, FIT, and Cologuard
The US Preventive Services Task Force now recommends that adults begin colorectal cancer screening at age 45 [24][25], with several effective options available:
- Colonoscopy: Often considered the gold standard, performed every 10 years. Beyond detection, colonoscopy allows for polyp removal during the same procedure, potentially preventing cancer development [10][25]. Studies show it can reduce colorectal cancer deaths by 50% among those who undergo the procedure [26].
- Fecal Immunochemical Test (FIT): A non-invasive stool test that detects hidden blood, performed annually [27][10]. While less invasive than colonoscopy, any positive result requires follow-up colonoscopy.
- Stool DNA tests: Products like Cologuard and Cologuard Plus combine FIT with tests that detect altered DNA from cancer or polyps [10][1]. The newer Cologuard Plus detected 92% of all colon cancers in clinical studies [28], with the advantage of at-home testing.
Patient adherence differs meaningfully between screening methods. Studies show 71% of patients complete Cologuard within 28 days versus only 42% adherence for FIT [1]. Higher adherence coupled with accurate testing significantly improves population-level outcomes.
Post-Treatment Monitoring and Recurrence Risk
Ongoing monitoring becomes an integral part of life after colon cancer treatment. Regular follow-up visits allow doctors to detect potential recurrences early and address treatment side effects.
CEA levels and imaging for recurrence detection
Carcinoembryonic antigen (CEA) serves as a valuable tumor marker for monitoring after treatment. For optimal surveillance, doctors recommend CEA testing every 3-6 months during the first two years, then every 6 months until five years post-treatment [14]. While CEA testing alone lacks sufficient sensitivity, it proves most effective for detecting liver metastases (80% sensitivity) and less reliable for lung recurrences (15% sensitivity) [14].
Imaging complements blood tests in surveillance protocols. CT scans of chest, abdomen, and pelvis typically occur every 3-6 months for the first two years for higher-risk patients, then every 6-12 months through year five [29]. Combined CEA and imaging detects recurrences more effectively than either method alone, with studies showing each method identifies roughly 30% of recurrences [14].
Surveillance colonoscopy schedule
Most physicians recommend the first surveillance colonoscopy approximately one year after surgery [30]. Assuming normal results, the next examination typically occurs three years later (four years post-surgery), followed by another at the nine-year mark [30]. Subsequent colonoscopies continue at five-year intervals unless diminishing life expectancy outweighs benefits [30].
Managing long-term side effects
Long-term side effects often persist after treatment completion. Common issues include:
- Bowel function changes: Some patients experience chronic diarrhea or difficulty controlling bowel movements [29]
- Peripheral neuropathy: Numbness or tingling in fingers and toes from chemotherapy [29]
- Ostomy adaptation: Patients with colostomies or ileostomies may benefit from enterostomal therapists who teach proper care techniques [29]
Communication with healthcare providers remains crucial, as many side effects can be effectively managed with appropriate intervention [31]. Some patients may need specialized support for radiation-related complications that emerge months or years after treatment [32].
Alternative and Supportive Therapies
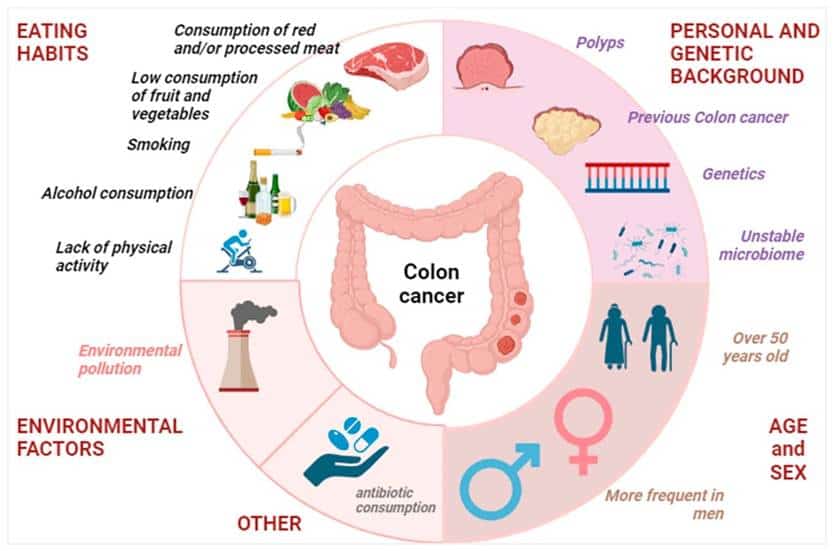
Image Source: MDPI
Many colon cancer patients explore approaches beyond standard medical treatments to support their journey. These additional therapies can play varying roles in managing symptoms and improving quality of life.
Is colon cancer curable in homeopathy?
Scientific evidence does not support homeopathy as a cure for colon cancer. Multiple studies have found no reliable evidence that homeopathic remedies can treat or prevent any type of cancer [13]. Notably, homeopathic products contain substances diluted to such a degree that often none of the original substance remains [33].
Homeopathy should never replace conventional cancer treatment. Doing so could delay effective therapy and harm health outcomes [33]. A study of cancer patients using alternative medicine instead of conventional treatments found they were nearly five times more likely to die after a median of 5 years [33].
Some patients use homeopathy alongside conventional treatment to manage side effects. Although limited research suggests potential benefits for chemotherapy-induced stomatitis or radiodermatitis [34], most studies are too small to draw firm conclusions [13].
Nutritional support and lifestyle changes
Proper nutrition plays a crucial role in cancer care, with malnutrition affecting up to 10-20% of cancer deaths [35]. Alongside conventional treatment, several lifestyle modifications may help reduce colorectal cancer risk:
- Diet: Focus on fruits, vegetables, and whole grains while limiting red and processed meats [36][37]
- Physical activity: Regular exercise links to reduced risk [36][37]
- Weight management: Maintaining healthy weight reduces risk factors [36][37]
- Hydration: Typically 8 glasses of water or low-sugar electrolyte drinks daily [38]
Palliative care for advanced stages
Palliative care aims to improve quality of life through symptom management and emotional support. Increasingly recognized as valuable, it can begin at any stage—not just end-of-life [39].
Palliative care provides several benefits including reduced time in intensive care units, improved quality of life, better emotional health, and potentially extended survival [39]. The multidisciplinary approach helps manage pain, nausea, fatigue, depression, and anxiety [40].
Primarily focused on alleviating symptoms, palliative care enables patients to live as fully as possible while managing their illness [41].
Conclusion
Colon cancer presents a unique public health challenge. While ranking as the third most common cancer diagnosis in the United States, it also stands as one of the most treatable when caught early. Throughout this article, we’ve seen how early detection transforms colon cancer from a life-threatening condition to a highly curable disease.
The evidence clearly demonstrates that localized colon cancer boasts an impressive 90% five-year survival rate. This number drops dramatically to just 13-14% once the cancer spreads to distant organs, therefore highlighting the critical importance of timely screening and diagnosis.
Perhaps most encouraging, the progression from polyps to malignant cancer typically spans 5-15 years, creating a substantial window for intervention. Regular screening through methods like colonoscopy, FIT tests, or newer options like Cologuard allows medical professionals to identify and remove precancerous polyps before they develop into tumors.
Treatment options vary significantly based on staging. Surgery alone cures approximately 95% of stage I cases, while stage III patients benefit from combination approaches involving surgery and chemotherapy. Even stage IV cancer offers potential curability in select cases, particularly when metastases remain limited and surgically removable.
Life after colon cancer treatment requires vigilance. Regular follow-up visits, CEA testing, and surveillance colonoscopies help detect potential recurrences early. Additionally, nutritional support and lifestyle modifications play important roles in both prevention and recovery.
The declining incidence and mortality rates from colon cancer over recent decades tell a powerful story about medical progress. Advances in screening technology, surgical techniques, chemotherapy, targeted therapies, and immunotherapy continue to improve outcomes across all stages.
Above all, these findings emphasize one crucial message: almost 60% of colorectal cancer deaths could be prevented with appropriate screening. When we detect colon cancer early, we dramatically increase the chances of complete cure and return to normal life expectancy.
Key Takeaways
Early detection of colon cancer dramatically transforms survival outcomes, with localized disease showing remarkable cure rates when caught in time.
• Early detection saves lives: Colon cancer caught in stages 1-2 has a 90% five-year survival rate, compared to just 13% for advanced disease.
• Screening prevents cancer: Polyps take 10-15 years to become malignant, creating a crucial window for detection and removal through colonoscopy.
• Surgery cures most early cases: Stage I colon cancer treated with surgery alone achieves 95% five-year disease-free survival rates.
• Start screening at 45: New guidelines recommend colorectal cancer screening beginning at age 45 using colonoscopy, FIT tests, or Cologuard.
• 60% of deaths are preventable: Almost two-thirds of colorectal cancer deaths could be avoided with appropriate screening and early intervention.
The key message is clear: colon cancer represents one of medicine’s greatest prevention success stories. When we catch it early through regular screening, what could be a devastating diagnosis becomes a highly treatable condition with excellent long-term outcomes.
FAQs
Q1. How effective is early detection in treating colon cancer? Early detection significantly improves colon cancer outcomes. When caught in stages 1-2, the five-year survival rate is around 90%, compared to only 13-14% for advanced stages.
Q2. At what age should I start getting screened for colon cancer? Current guidelines recommend starting colorectal cancer screening at age 45 for people at average risk. However, those with a family history or other risk factors may need to start earlier.
Q3. What are the most common symptoms of colon cancer? Common symptoms include changes in bowel habits, blood in stool, persistent abdominal discomfort, unexplained weight loss, and fatigue. However, early-stage colon cancer often has no symptoms, which is why regular screening is crucial.
Q4. Can colon cancer be cured if caught early? Yes, colon cancer has high cure rates when detected early. For stage I colon cancer, surgery alone can achieve a 95% five-year disease-free survival rate.
Q5. What screening methods are available for colon cancer? Several effective screening methods exist, including colonoscopy (recommended every 10 years), annual Fecal Immunochemical Tests (FIT), and stool DNA tests like Cologuard. Your doctor can help determine the best option for you based on your risk factors and preferences.
References
[2] – https://cancer.ca/en/cancer-information/cancer-types/colorectal/signs-and-symptoms
[3] – https://www.moffitt.org/cancers/colon-cancer/survival-rate/
[5] – https://www.cancer.org/cancer/types/colon-rectal-cancer/treating/by-stage-colon.html
[7] – https://www.massgeneralbrigham.org/en/about/newsroom/articles/stage-4-colorectal-cancer
[9] – https://pmc.ncbi.nlm.nih.gov/articles/PMC7564362/
[11] – https://www.mdanderson.org/cancerwise/is-colon-cancer-curable.h00-159616278.html
[12] – https://www.mayoclinic.org/diseases-conditions/colon-cancer/symptoms-causes/syc-20353669
[14] – https://www.cancernetwork.com/view/cea-monitoring-colorectal-cancer
[16] – https://my.clevelandclinic.org/health/diseases/14501-colorectal-colon-cancer
[17] – https://www.medicalnewstoday.com/articles/stage-3-colon-cancer
[18] – https://www.mayoclinic.org/diseases-conditions/stage-4-colon-cancer/diagnosis-treatment/drc-20584817
[19] – https://wjso.biomedcentral.com/articles/10.1186/s12957-021-02207-4
[20] – https://pmc.ncbi.nlm.nih.gov/articles/PMC10486610/
[21] – https://oncodaily.com/oncolibrary/immune-oncology/immunotherapy-for-colon-cancer
[22] – https://pmc.ncbi.nlm.nih.gov/articles/PMC6791134/
[23] – https://pmc.ncbi.nlm.nih.gov/articles/PMC11271734/
[24] – https://www.cdc.gov/colorectal-cancer/screening/index.html
[25] – https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/colorectal-cancer-screening
[27] – https://medlineplus.gov/ency/patientinstructions/000704.htm
[28] – https://www.cologuard.com/faq
[29] – https://www.cancer.org/cancer/types/colon-rectal-cancer/after-treatment/living.html
[30] – https://gastro.org/clinical-guidance/colonoscopy-surveillance-after-colorectal-cancer-resection/
[32] – https://www.cancer.gov/about-cancer/coping/survivorship/late-effects
[33] – https://www.verywellhealth.com/homeopathic-remedies-for-cancer-88905
[34] – https://www.sciencedirect.com/science/article/abs/pii/S0959804905009962
[35] – https://pmc.ncbi.nlm.nih.gov/articles/PMC9180662/
[36] – https://nyulangone.org/conditions/colorectal-cancer/prevention
[37] – https://www.cancer.org/cancer/latest-news/six-ways-to-lower-your-risk-for-colon-cancer.html
[38] – https://www.cancercenter.com/community/blog/2021/05/colon-cancer-diet
[39] – https://www.cancer.org/cancer/supportive-care/palliative-care.html
[40] – https://colorectalcancer.org/resources-support/resources/palliative-care
